
This month marks the 50th anniversary of the LGBTQ Pride tradition. The first Pride celebration, held in 1970, commemorated the Stonewall Uprising where thousands of protestors gathered at the Stonewall Inn to speak out against police brutality and systemic discrimination. These issues remain relevant today, and Pride 2020 has focused on supporting Black Lives Matter and raising awareness about the inequities imposed on racial and sexual minorities in the United States.
One such inequity is the prevalence of health disparities that can affect quality of life and life expectancy, and are often intersectional. Obesity is a prime example of intersectionality in health disparities. Black American adults experience higher obesity rates then white Americans (49.6% vs 42.2%), but when prevalence is broken down by gender, the disparity among women is even greater- 56.9% for Black women compared to 39.8% for white women. When gender and sexual orientation are considered, lesbians are 49% more likely, and bisexual women are 43% more likely than heterosexual women to have obesity.
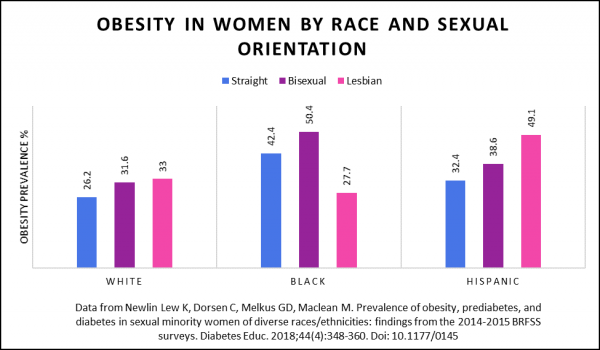
As shown in the figure below, data from the Behavioral Risk Factor Surveillance System (BRFSS) indicated that Black bisexual women experienced the highest rates of obesity and Hispanic lesbians had the highest rates of diabetes. Notably, white and Hispanic women experienced greater obesity rates if they were lesbian or bisexual, while Black lesbians experienced lower rates of obesity than their straight counterparts. Because heights and weights in the BRFSS are self-reported, these data underestimate the true prevalence of obesity.
Although the causes of obesity are diverse and complex, systemic factors like discrimination and lack of access to adequate healthcare are likely at the root of these health disparities. Minority stress can play a role, as well as policies that disadvantage minorities in employment, housing, and public accommodations. Until recently, the majority of U.S. states did not offer protection against workplace discrimination for LGBTQ employees. As a result, members of the LGBTQ community are more likely to be unemployed, experience food insecurity, and lack health insurance. This disparity in employment has increased during the current pandemic, with 17% of LGBTQ respondents and 22% of LGBTQ respondents of color compared to 13% of heterosexual respondents reporting unemployment as a result of COVID-19.
This month two federal actions changed the landscape of health in the LGBTQ community. On June 12th the Trump administration finalized a rule that ends the inclusion of sexual orientation and gender identity in protections against sex discrimination in health care and health insurance. Opponents of this rule fear that it will decrease health care utilization among the LGBTQ population, especially transgender individuals. Just three days later, the Supreme Court ruled that the Civil Rights Act protects against workplace discrimination on the basis of sexual orientation or gender identity. This federal ruling ensures that LGBTQ individuals are protected from workplace discrimination regardless of whether their state offers explicit protections.
Reducing health disparities will require addressing systemic inequities through policies that increase access to health care and eliminate discrimination in housing and the workplace. Additionally, more research is needed to explore the effects of intersecting identities on health. Sexual orientation and gender identity should be included as demographic variables in obesity research and these variables should be included in analyses that compare prevalence rates between groups. Understanding the way that race, sex, and sexual orientation intersect to affect the risk of obesity across populations must be done to ensure equity in obesity care.