
November is National American Indian and Alaska Native Heritage Month. American Indian/Alaska Natives (AI/ANs) make up 1.7% of the total U.S. population. In 2019, an estimated 5.7 million people identified as AI/AN alone or in combination with one or more other races.
AI/ANs experience one of the highest rates of obesity across all racial and ethnic groups in the United States. In 2018, 48.1% of AI/AN adults aged >18 years old had obesity. AI/AN adults are approximately 60% more likely to have obesity than non-Hispanic White adults. AI/ANs also experience disparities in mortality rates. AI/AN individuals born in 2019 have a life expectancy that is 5.5 years less than the U.S. average for all races (73.0 years versus 78.5 years). AI/AN populations experience higher mortality rates due to obesity-related conditions, such as heart disease, diabetes, stroke, and chronic liver disease and cirrhosis compared to all U.S. races.
Children who identify as AI/AN have consistently experienced higher rates of both overweight and obesity compared to White children. In 2015, 29.7% of AI/AN children aged 2 to 19 years had obesity, whereas in 2015-2016, 14.1% of non-Hispanic White children aged 2 to 19 years had obesity. Among children ages 2 through 4 enrolled in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) in 2016, AI/AN children experienced a much higher prevalence of overweight and obesity compared to Non-Hispanic White children, as demonstrated in the figure.
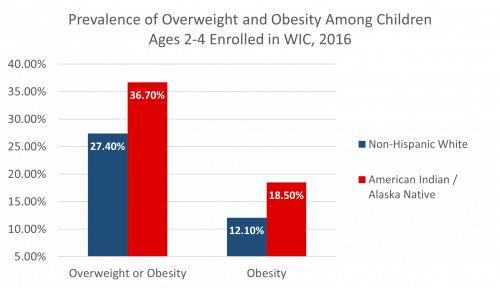
Source: Graph adapted from Pan et al., 2019
Various upstream factors have contributed to the disproportionately high rates of obesity in AI/AN communities. Historically, the forced relocation of AI/AN peoples away from their ancestral lands and onto reservations severely restricted their access to traditional, regionally-specific food systems such as hunting, gathering, fishing, and farming. Many tribes were agriculturalists and originated the concept of regenerative agriculture. One example is seen in the Iroquois’ cultivation of the “Three Sisters” (corn, beans, and squash). This disruption of indigenous food systems by colonizers has resulted in dependence on federal government programs which include unhealthy foods. While AI/AN communities have adapted to these systemic changes by inventing new “traditional” foods such as fry bread, inconsistent funding for food assistance programs and other social services continue to contribute to food insecurity. Today, AI/AN tribal area populations are mostly rural and experience high rates of poverty, restricting geographic and economic access to food.
AI/ANs also face barriers in accessing and navigating health care services, including the geographical isolation of rural areas, costs of travel, and/or lack of access to transportation. This population also experiences higher rates of unemployment and poverty and lower rates of insurance coverage compared to other races. In addition to these disparities, inadequate funding of the Indian Health Service (IHS) contributes to staff shortages and prolonged wait times in IHS clinics.
To increase health equity for AI/AN communities, stakeholders must recognize and address the lasting impact of historical trauma and systemic racism, while honoring the strength and resiliency of AI/AN communities. Specific actions to improve the health and reduce obesity of AI/AN communities include the implementation of community-based participatory research and culturally relevant programs to promote local food production and increase food security. These steps include promotion of food sovereignty, embracing indigenous diets, improving access to traditional foods, promotion of early childhood nutrition through culturally tailored programs, taxation of unhealthy foods and subsidization of healthier options, increasing funding for the IHS, and increasing tribal control of health programs and services. In addition to these actions, public health efforts can also include the restoration of cultural traditions of physical activity, such as running long distances, to help prevent and control the prevalence of obesity and other chronic diseases.
The pursuit of health equity for AI/ANs is a complex effort that requires a multipronged approach. For more information on AI/AN health disparities and proposed solutions, you may view our new fact sheet here.